About Palmoplantar Pustulosis
Palmoplantar Pustulosis
➢ What is palmoplantar pustulosis (PPP)?
Palmoplantar pustulosis (PPP) is a type of skin disease that is characterized by repeated eruptions of multiple small pustules on the palms of the hands and soles of the feet. Although these small vesicles are filled with pus, the pus is sterile (it is “sterile” because no infection is observed).
Since patients often feel an itching sensation when the blisters are forming, it may be misdiagnosed at first as roughness of the hands or athlete’s foot. However, topical treatment often fails to alleviate the symptoms.
As the pus-filled vesicles form repeatedly on the skin, the affected area of the skin also expands.

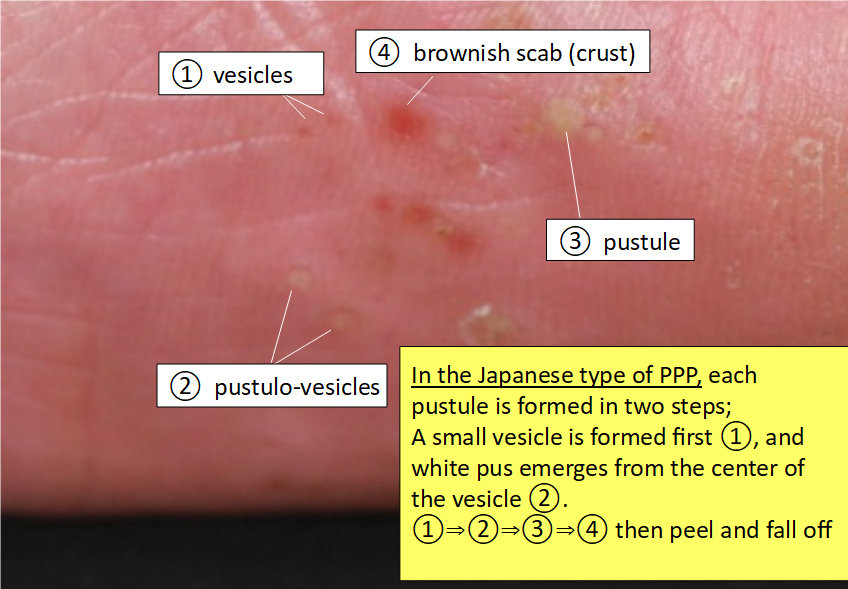
Pustules (white), vesicles and scab (reddish brown) on the palm
The disease is not contagious. Since the pus is sterile, the disease is not transmissible by contact. Due to the poor awareness of the general population of PPP as a non-contagious disease, there could be a stigma attached to the disease, and people may avoid coming in contact with patients with PPP for fear of becoming infected. Thus, patients with PPP are sometimes hurt by the thoughtless remarks and inconsiderate behaviors of others. Some patients always wear gloves, do not go to pools or hot springs, and feel depressed on account of fear of such rejections.
Some patients are unable to walk or use their hands due to pain, and some others reveal acute severe chest pain. If there are multiple pustules on the palms of the hands and soles of the feet, it can significantly impair the patient activities of daily living (including inability to walk due to pain, difficulty with washing face/hair, grocery shopping, cooking, etc.). The disease causes significant deterioration of health-related quality of life (HR-QOL).
Furthermore, 10-30% of patients also manifest inflammation of the clavicle, sternum, spine. In some cases, the patients suffer from sudden onset of severe chest pain, which could be mistaken for angina pectoris or myocardial infarction.
Symptoms of hands and feet
A characteristic symptom of PPP is the development of pustules, consisting of small vesicles on the palms of the hands and soles of the feet (planta).
Although pustules on the hands and feet can develop in other conditions, the pustules of PPP have characteristic features.
In the Japanese type of PPP, each pustule of PPP is formed in two steps: A small vesicle is formed first, and white pus emerges from the center of the vesicle. Although all inflammation is caused by white blood cells (probably monocytes), the white blood cells responsible for the initial inflammation are different from those responsible for the white pustules (neutrophils) (refer to What causes palmoplamtar pustulosis (PPP) and Pathogenesis on palmoplantar pustulosis).
Since the vesicles are very small, patients often detect them only when they feel the itching sensation during the formation of the vesicles. A short time after a vesicle becomes a white pustule, it becomes dry, followed by the formation of a brownish scab, which is easily noticeable.
Cited and modified from the article by Satomi Kobayashi, Rinsho Derma, Vol. 60 (2018) (*3)
After a few days, as the skin underneath the lesion starts healing, the skin lesion along with the surrounding stratum corneum (white crust called “scale”) peel off spontaneously and fall off. The area of the affected skin then looks red (erythema) and dry.
After a few repetitions of the same process on the palms of the hands and soles of the feet, a diffuse area of the skin turns red and dry. The palms of the hands and soles of the feet look red, covered with pustules, scabs and peeling off skin.

When many layers of the stratum corneum pile up, the skin loses its elasticity and cracks. Cracking of the skin causes pain. If the entire soles of the feet become covered with skin eruptions, it becomes impossible to walk due to pain. Some patients have described feeling as if they are walking on broken glass shards or pushpins.
You need to monitor frequency of pustule formation
In the Japanese type of PPP, when new pustules form continuously, it is necessary to find out if there is any hidden trigger factor for the PPP, for example, focal infections such as tonsillar lesions or odontogenic focal infection. (refer to “What causes palmoplantar pustulosis (PPP)?” / “Treatment for PPP”).
Attention should be paid to any discomfort or swelling in the throat or gingiva when you are tired and to possible aggravation of symptoms with a cold. If you notice any such condition, you need to inform your attending physician.
The skin symptoms may not improve for decades with only topical treatment. Even if the skin symptoms do improve after high doses of oral biotin for many years, PPP can subsequently progress to bone or joint symptoms if a hidden lesion or focal infection is left untreated.
Smoking can be one of the major trigger factors for the onset of PPP, even the non-Japanese type.
In cases of PPP, pustules often form in a recurrent and periodic fashion. This is presumably attributable to the interaction between the immune reactions causing pustule formation and the immune reactions directed at suppressing the pustule formation.
The pustules often relapse and disappear in cycles of approximately 4 weeks. Even during the period of a single cycle, trigger factors (such as tonsillar or odontogenic infection, or chronic infections including sinusitis) are frequently observed in many cases with the Japanese type of PPP. When the cycle is shorter (for example, pustules relapsing every 1-2 weeks), you need to consult a physician for a thorough search of any asymptomatic focal infection.
If a trigger factor is identified, its treatment or removal usually results in improvement of the lesions within 6 months or so. In 60-80% of patients with the Japanese type of PPP, the skin symptoms usually resolve completely within 1-2 years.
Are you psychologically stressed or overworked?
Immune status also affects the onset/course of the pustules in cases of PPP.
When a person experiences significant psychological stress or pushes him/herself physically (overwork), the number of pustules tends to increase.
Focal infection in cases of PPP is often caused by the commensal bacteria in the nose, throat or mouth (teeth). The normal flora are usually non-pathogenic, coexisting harmlessly with us. When the immune system becomes unstable because of excessive stress or fatigue, however, autoinflammation reacts with dysbiosis and may trigger an excessive immune response (breakdown of immune tolerance).
Palmoplantar pustulosis aggravates with touching or rubbing
Peeling and dried skin (scales) is not only annoying, but can also cause pain. Dry and stiff scales can irritate the skin when a person is standing or walking. You may want to peel off and smoothen the skin to avoid such irritation. However, since PPP aggravates with such mechanical stimuli (Köebner phenomenon), such a tendency should be avoided (refer to “Treatment for PPP”).
The stratum corneum of the palms and soles is significantly thicker than that of other parts of the skin, and takes a longer time to repair. Rubbing and peeling of the skin interfere with return of the skin to a flat and smooth condition. Therefore, the urge to peel of scales should be resisted, and one must wait for the skin to spontaneously heal. You can prevent drying of the skin and keep the skin moisturized with ointments. Zinc oxide ointment can protect the skin from irritation. Rubbing an ointment into the skin must also be avoided (refer to “topical treatment”).
❐ Skin symptoms in areas other than the hands and feet – extra-palmoplantar eruptions –
In some cases, erythematous areas may appear on the elbows, knees, forearms and lower legs. Although the erythematous areas may resemble those of psoriasis, they have less well defined borders and show milder induration as compared to the lesions of psoriasis in Japanese patients.
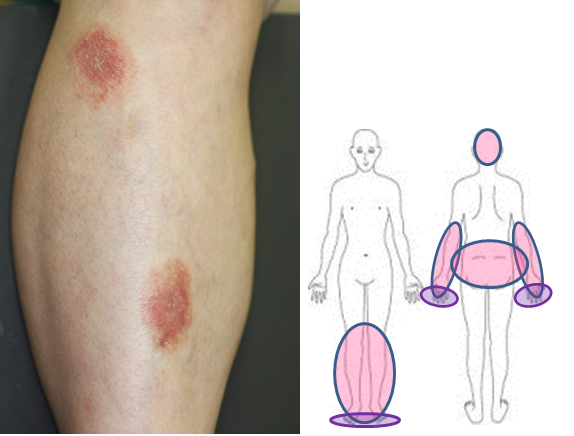
Exstra- palmoplantar eruptions and their distribution
These eruptions are also different from those of psoriasis histopathologically, and are called extra-palmoplantar eruptions. Extra-palmoplantar eruptions can be observed even on the scalp and buttocks, and might be mistaken for eczema and folliculitis in the case of lesions on the scalp or for tinea in the case of lesions on the buttocks. These lesions are often itchy. Since information on the clinical condition will help in the diagnosis (i.e., persisting for a few months and not responding to topical treatment), we strongly recommend that you provide accurate information to your attending physician.
Nail symptoms
Nail manifestations include pustulation under the nail plate, pitting, destructive changes, thickening of the nail or of the skin under the nail plate, and nail discoloration. The changes may lead to nail detachment.

Pustules under nail plate

Thickening of nail plate

Difficulty in performing tasks using the fingertips due to pain associated with destructive changes of the nails.
Nails are normally visible to everyone, and the aforementioned nail manifestations can lead to depression. Furthermore, broken nails can catch the hairs or clothing fabrics. When the nails are destroyed, it is difficult to pick up things like thin coins. Thus, the nail manifestations can lead to significant impairment of the daily living activities.
These manifestations can improve with appropriate treatments. The attending physician should be informed of all the problems and inconveniences, and should be consulted about the treatments that are available.
Most outpatient dermatology clinics/hospitals are very busy, and a patient may feel hesitant to ask such questions. In such cases, the problems can be explained to the nurses. The attending physician may be given a list of the matters of concern to be discussed at a subsequent visit. This will give the physician an opportunity to consider treatment options appropriate for individual patients.
Characteristic sternoclavicular arthritis
The sternum, clavicles, joints between the sternum and the first rib, and the rib junctions on the upper and lower sternum are considered as characteristic sites of joint involvement in PAO. About 80% of patients with PAO manifest bone lesions in the anterior chest wall.

Chest wall swelling is observed
Since the patients may develop sudden severe pain around the neck to the chest, the condition is sometimes misdiagnosed as angina pectoris, myocardial infarction or reflux esophagitis.
The sternoclavicular region moves with breathing. Therefore, even breathing can be painful, and coughing and sneezing entail great pain.
Turning over in bed may cause significant pain. Therefore, many patients have a problem sleeping on their beds, and often doze while leaning against a couch.
Even X-rays may not confirm the diagnosis, because the bone changes of osteoarthritis do not occur immediately.
❐ Pustulotic arthro-osteitis: PAO and SAPHO syndrome
PAO is also sometimes called the Synovitis, Acne, Pustulosis, Hyperostosis, Osteitis (SAPHO) syndrome. The SAPHO syndrome covers approximately 50 terms of diseases, including PAO, acne spondyloarthritis, chronic recurrent multifocal osteomyelitis (CRMO), diffuse sclerosing osteomyelitis of mandible, enteropathic spondyloarthritis. PAO accounts for most cases of SAPHO syndrome in Japanese patients, and has been reported to account for 52-56% of cases of SAPHO syndrome in the world.
However, the underlying PPP has a characteristic feature, that of focal infection as the trigger of the onset of the disease in 60~80% of Japanese patients, which is directly related to the treatment strategy of PAO. In order to stay aware of the importance of eliminating the trigger in the treatment, it is important to treat PAO individually, without considering it under the umbrella of SAPHO syndrome.
The therapeutic approach to SAPHO syndrome also remains unsatisfactory. By analyzing the diseases individually, it may become clear which treatment must be prioritized .
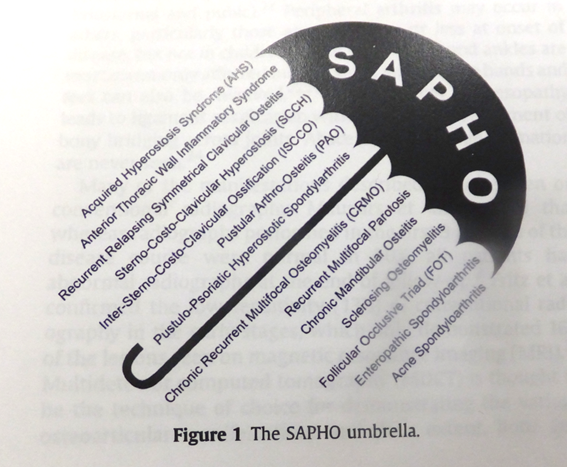
Sited from Depasquale R, et al. SAPHO: What radiologists should know. Clin Radiology 67, 2012
❐ Attention must be paid to pain in the neck, back and lower back
PAO can involves various areas. Inflammation can occur in the neck, spine spine (spondylitis, arthritis of sacroiliac joints), shoulders (arthritis of acromial joints) and hip joints, as well as in the bones and joints of the hands and feet (peripheral arthritis).
The spine bears much of the body weight, and weakening of the spine due to inflammation may cause spinal fractures. Therefore, patients should not take it lightly as mere back pain, but inform their attending physician.
If pain is felt in the soles or heels of the feet, it may be attributed to enthesitis in the major tendons or ligaments that are continuously used on a daily basis. Enthesitis is an inflammation of the entheses (the sites of insertion of tendons and ligaments into bones).

Bamboo spine of the neck

Peripheral arthritis. Swelling are observed on the feet.
Furthermore, osteitis due to PPP can also be observed in the bones of the long bones in extremities (aseptic osteomyelitis).
Bone inflammation is normally accompanied by severe pain.
In such cases, accurate diagnosis is very important. It is necessary to differentiate the pain from that caused by bone metastasis (metastatic cancer) and bone infections due to conventional bacteria or other bacteria such as Mycobacterium tuberculosis.

Bone scintigraphy. Inflammation is observed in femur.
What types of examinations should be performed?
There are several examinations for osteoarthritis. The following examinations should be performed on an as-needed basis in order to make a diagnosis, study the current status of inflammation, and determine whether or not the condition is complicated by other bone diseases causing pain. Based on findings of the examinations, a comprehensive judgement is made on what kind of treatment is necessary.
Laboratory examination (blood test)
Acute- and chronic- phase reactants are measured for evaluation of the inflammation. Laboratory examinations are also performed in order to determine the presence of autoantibodies, including rheumatoid factor and antinuclear antibody for differential diagnosis, and to search for comorbidities, including autoimmune thyroiditis, diabetes, hyperlipidemia and other immunological disorders.
Plain radiography
Plain X-rays are the standard radiographs for bones. The types of bone changes can be evaluated, and any cause of lower back pain other than the normal aging process is searched for.
MRI STIR sequence/fat suppressive image
Magnetic resonance imaging (MRI) is the most effective method to identify the bone lesions of PAO. A short tau inversion recovery (STIR) sequence or fat suppressive T2W1 image will not only show bone inflammation as accurately as bone scintigraphy, but also provide further pathoanatomical details. T1W1 imaging will show bone changes of inflammation, such as bone erosion and bone proliferation, and signs of past inflammation such as fat deposition in the bone or ankylosing changes. T2W1 imaging is also used to detect inflammation, however, STIR or fat suppressive imaging is needed to detect PAO lesions. In addition, MRI has the advantage of not exposing a patient to any inherent radiation risk.

Left: fat suppressive image. Inflammation sites are edematous and looks whitish.
Right: T1W1 image. Vertebral bones show constructive fracture in multiple locations.
- Bone scintigraphy
- In patients presenting with pain in various parts of the body, it is often difficult to find the site of inflammation. Bone scintigraphy, however, allows all sites of bone inflammation in the body to be identified at the same time. Bone scintigraphy does not help in identifying changes in the forms/shapes of bones.
Pulse-echo ultrasound
In arthritis of the wrist, ankle and elbow joints, pulse-echo ultrasound shows vascular proliferation during the early phase of inflammation. Since swelling and bone proliferation due to inflammation can be monitored without radiation exposure, it is a safe and convenient clinical tool.
❐ Subtypes and terminology of palmoplantar pustulosis (PPP)
PPP was first defined in the 1930s. Two different types are recognized, and their terminology and skin manifestations have been under debate for 30 years. In 1961, the name “pustulosis palmaris et plantaris (PPP)” was adopted. At present, two subtypes of PPP are recognized, and the Japanese type, which is related to focal infections seems to be different from that encountered in Western countries, and another type which is a localized type of pustular psoriasis that is not seen in Japanese.
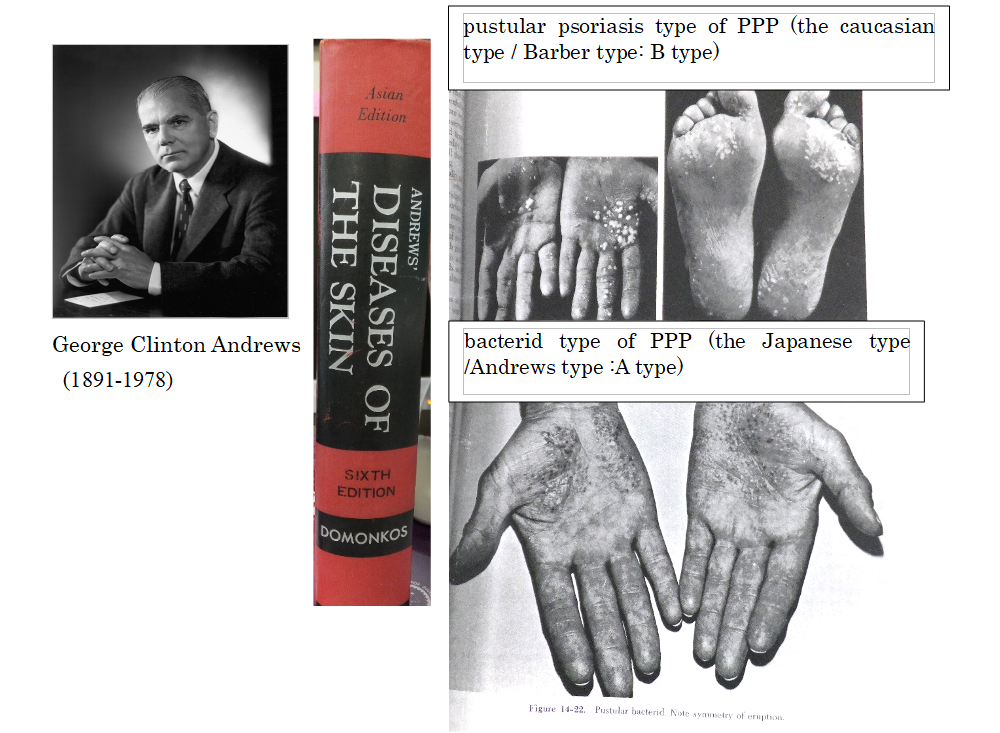
In 1930, Barber and Ingram advocated use of the term “pustular psoriasis of the extremities” to refer to psoriatic pustular reactions of the hands and feet. In 1934-1935, Andrews defined “pustular bacterid” as “pustular eruptions of the palms of the hands and soles of the feet that do not respond to topical treatment, but potentially resolve with tonsillectomy and/or dental treatment, as it is closely related to tonsillar and dental conditions”; this is the Japanese type of PPP. He thoroughly examined the two conditions, and stated in his textbook that the bacterid type of PPP (image on the bottom right) completely differs from the pustular psoriasis type of PPP (image on the upper right) in respect of the way in which the skin rashes develop. The skin rash in the pustular psoriasis type is a pustule from the beginning, while the skin rash in the bacterid type is a vesicle at first, that subsequently becomes a pustule. In other words, these two types of disease develop with completely different onset mechanisms, and the causes are also different. Focal infections of tonsil and periodontitis are only involved in the onset of bacterid type, Japanese type of PPP.
❐ What needs to be done for PPP
The prevalence rate of PPP is considered to be the highest in Japan. The national prevalence of PPP in Japan is approximately 0.12%, and the number of Japanese patients with PPP is estimated to be 135,000. These patients suffer from skin symptoms on the important functional sites of hands and feet, and severe pain associated with pustulotic arthro-osteitis (PAO), which often causes impairment of daily living activities. Therefore, efforts have been started to establish standard treatments and to develop new treatment methods by reviewing research data accumulated to date in light of progress in understanding of the immunology of the disease.
While PPP observed in western countries is localized pustular psoriasis, it is also a refractory chronic disease. Localized pustular psoriasis-type PPP can be complicated by arthritis and is called the SAPHO syndrome. Pustular psoriasis is in itself intractable, and generalized pustular psoriasis is registered as an intractable disease by the Japanese Ministry of Health, Labour and Welfare.
Development of new systemic therapies including biologics (injection and oral preparations) has advanced at a rapid pace in recent years. Considering the fact that there are 2 different types (subtypes) of PPP (the Japanese type and the caucasian type), it is important that doctors recognize and understand the other type of PPP, and assess the safety and effectiveness of each treatment while determining if each treatment is specifically effective against either type or effective against both types.
❐ Japanese type of PPP
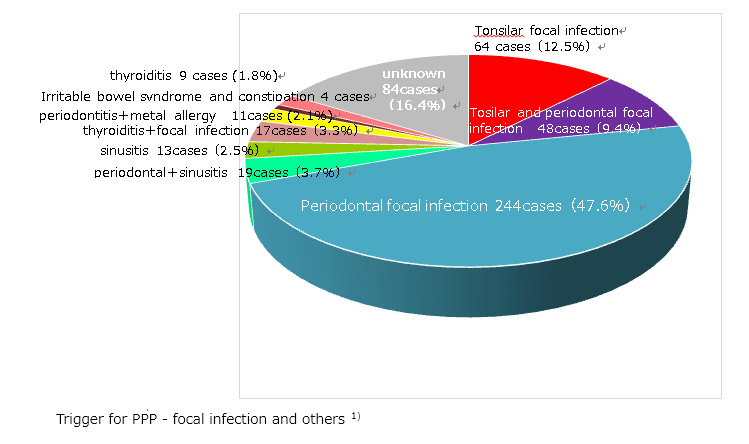
As we examine the findings of Andrews or past Japanese dermatologists, patients with PPP, it is evident that standard treatments (such as topical therapy and phototherapy) have insufficient effect in most patients. More than 80% of Japanese patients with PPP have asymptomatic focal infections in the mouth, such as periodontitis, tonsils or nasal sinuses1) , and treatment of these asymptomatic foci of infection has been observed to lead to resolution of the skin symptoms in more than 60-80% of the patients1-4)
On the other hand, PPP in Europeans and Americans resembles a type of psoriasis (pustular psoriasis in the extremities –Barber and Ingram-), which manifests pustules on the palms and soles, as well as pustules or psoriatic lesions on the arms and lower extremities. It is rare to be related with focal infections in this type of PPP.
These differences may be the reason for difficulty of understand the other side of PPP, resulted in the delay of establishing treatment strategies for them.
Another possible reason for the delay in the establishment of treatment for this condition is that the mechanism underlying its relation with “focal infection” is unknown. However, some evidences have been accumulated. PPP patients show a hyperimmune response to indigenous bacteria such as a-streptococci, due to impaired immunological tolerance towards such organisms 5) . Such a novel immune response leads to T-cell activation through the abnormal expression of secondary stimulation molecules, including cytotoxic T-lymphocyte-associated antigen 4, inducible T-cell co-stimulator and Smad7, in the tonsils of PPP patients. Activated tonsillar T cells express cutaneous lymphocyte antigen (CLA), CCR6 and β1-integrin, enter the blood circulation and are recruited to PPP skin lesions6) .
Regardless of above, no biomarkers have been established, and dermatologists, laryngologists and dentists have not yet arrived at a consensus as to how to handle asymptomatic foci of infection to date. But still, the Japanese type of PPP is expected to be cured by treatment of asymptomatic focal infections, including prevention of progression to arthro-osteitis.
1)Kobayashi S. Diagnosis and treatment for PPP. Rinsho Derma 2018; 60 (10): 1539-1544 (Japanese)
2)Clinical Characteristics of Japanese Patients with Palmoplantar Pustulosis. Yamamoto T.
3)Yamamoto Y, et al. Effects of treatment for dental focal infection on pustulosis palmaris et plantaris. Jpn J Dermatol 2001; 111: 821-826 (Japanese)
4)Murakata H, et al. Increased interleukin-6, interferon-gamma and tumor necrosis factor-alpha production by tonsillar mononuclear cells stimulated with alpha-streptococci in patients with pustulosis palmaris et plantaris. Acta Otolaryngol 1999; 119:384-91
5)Harabuchi Y, Takahara M. Pathogenic role of palatine tonsils in palmoplantar pustulosis:A review. J Detrmatol 2019; Sep doi: 10.1111/1346-8138.15100
6)Clin Drug Investig. 2019 Mar;39(3):241-252. doi: 10.1007/s40261-018-00745-6.
Yes, it is true. The prevalence is high in the Japanese and Swedish, and relatively high in Chinese and Koreans.
The prevalence of a disease may vary among countries. One of the speculated reasons is the differences in the human leukocyte antigen (HLA) profile.
HLA determines whether or not rejection would occur at the time of organ transplantation, and decides how the immune system responds to each foreign object, such as bacteria or viruses. The HLA system is a gene complex that is responsible for the diversity of immune responses.
The susceptible HLA type for PPP has not yet been identified. About 5-6% of patients with PPP have a family member (parent, sibling or relative) with the same disease. However, HLA is like immunological predisposition passed on from generation to generation, and there is an extremely large number of HLA patterns. It is unnecessary to worry about passing PPP to children.
Identification of the susceptible HLA type for PPP may help in determining why such immune responses occur, why focal infection is a strong trigger factor in Japanese patients with PPP, and how to treat the condition in the future.
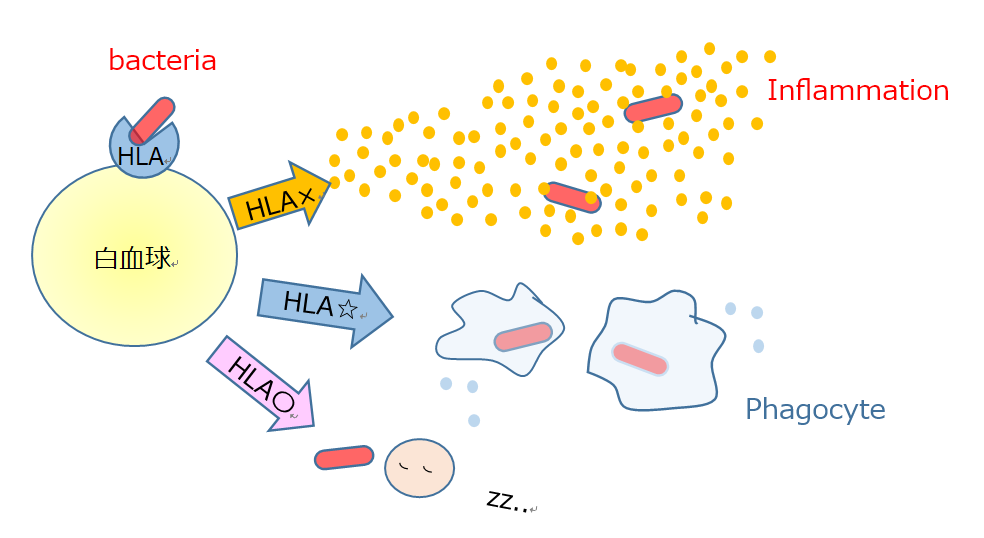
HLA and diversity of immune response
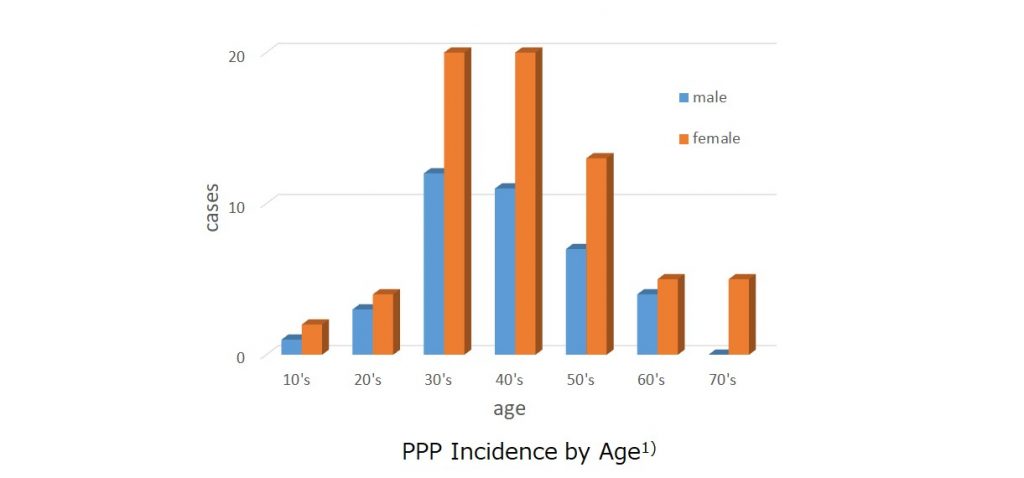
❐ The male: female ratio of PPP is about 1:2, and women in their 30s to 50s are more susceptible to PPP.
Statistics from various institutions in Japan have indicated a predisposition of middle- aged women for this disease.
In a study of PPP conducted in the year 2010 in response to a request from national health insurance societies throughout Japan, the male:female ratio was found to be around 1:2, and the incidence rate was the highest among patients in their 30s to 50s.
The number of patients with PPP in Japan is estimated to be 135,000, and the calculated prevalence rate is 0.12%.
The disease is rarely encountered in children.
1. Fujishiro K, et al. The Japanese Journal of Dermatology, 2015; 125: 1775-1782
2. Kubota K, et al. Epidemiology of psoriasis and PPP: a nationwide study using the Japanese national claims database. BMJ Open, 2015: 5: e006450. Doi: 10.1136/bmjopen-2014-006450
3. Akiyama T, et al. The relationships of onset and exacerbation of pustulosis palmaris et plantaris to smoking and focal infections. J Dermatol. 1995; 22: 930-934
❐ Pustules and bone pain occur simultaneously in most cases
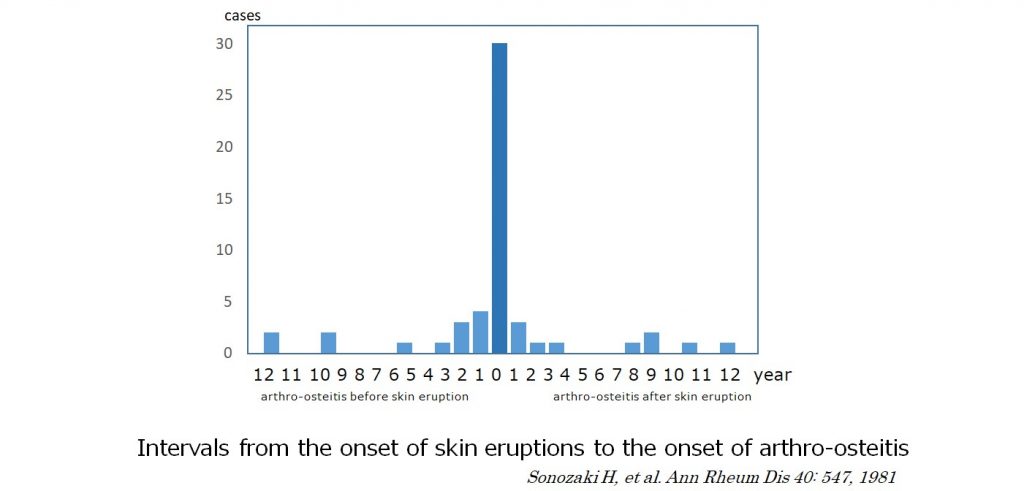
Sonozaki H, et al. reported that pustulotic arthro-osteitis (PAO) is most often observed in the anterior chest wall (sternoclavicular arthritis of the clavicle, sternum and ribs), shoulders, spine and various other parts of the body, and that more than 70% of the patients develop pustulosis and PAO simultaneously within 2 years difference. On the contrary, 80% of psoriasis patients develop skin lesions before psoriatic arthritis. Furthermore, there were cases that showed pustulosis many years after the occurrence of arthro-osteitis. In patients with pustules on the palms and soles, chest or back pain may be suspected to be caused by pustulotic arthro-osteitis. On the other hand, in patients presenting with back pain alone, it could take many years before an accurate diagnosis is made.
It is important to suspect the possibility of PAO in patients with pain in the chest wall or back without any obvious cause. If it is “pain at rest” (the patient experiences the most severe pain when waking up in the morning or after prolonged rest), the attending physician must be notified.
In PAO, the pain may resolve and recur repeatedly. To confirm the diagnosis, radiological examination is necessary.